Cancer Epidemiology, Biomarkers & Prevention | Research on Curcumin
Abstract
Curcumin, a constituent of the spice turmeric, has been shown to reduce the adenoma burden in rodent models of colorectal cancer accompanied by a reduction of levels of the oxidative DNA adduct 3-(2-deoxy-h-di-erythro-pentafur-anosyl)-pyr[1,2-A]-purin-10(3H)one (M1G) and of expression of the enzyme cyclooxygenase-2 (COX-2). We tested the hypothesis that pharmacologically active levels of curcumin can be achieved in the colorectum of humans as measured by effects on levels of M1G and COX-2 protein. Patients with colorectal cancer ingested curcumin capsules (3,600, 1,800, or 450 mg daily) for 7 days. Biopsy samples of normal and malignant colorectal tissue, respectively, were obtained at diagnosis and at 6 to 7 hours after the last dose of curcumin. Blood was taken 1 hour after the last dose of curcumin. Curcumin and its metabolites were detected and quantitated by high-performance liquid chromatography with detection by UV spectrophotometry or mass spectrom-etry. M1G levels and COX-2 protein expression were measured by immunoslot blot and Western blotting, respectively. The concentrations of curcumin in normal and malignant colorectal tissue of patients receiving 3,600 mg of curcumin were 12.7 F 5.7 and 7.7 F 1.8 nmol/g, respectively. Curcumin sulfate and curcumin glucuronide were identified in the tissue of these patients. Trace levels of curcumin were found in the peripheral circulation. M1G levels were 2.5-fold higher in malignant tissue as compared with normal tissue (P < 0.05 by ANOVA). Administration of curcumin (3,600 mg) decreased M1G levels from 4.8 F 2.9 adducts per 107 nucleotides in malignant colorectal tissue to 2.0 F 1.8 adducts per 107 nucleotides (P < 0.05 by ANOVA). COX-2 protein levels in malignant colorectal tissue were not affected by curcumin. The results suggest that a daily dose of 3.6 g curcumin achieves pharmacologically efficacious levels in the colorectum with negligible distribution of curcumin outside the gut. (Cancer Epidemiol Biomarkers Prev 2005;14(1):120 – 5)
Introduction
A shortcoming of the clinical development of many cancer chemopreventive agents has been the lack of knowledge, before the design of long-term phase II intervention trials, of the relationship between markers of pharmacologic activity and levels of agent required for efficacy. For example, the absence of robust pharmacokinetic information for h-carotene at the trial design stage has been implicated as one potential reason for the disappointing outcome of two large lung cancer prevention trials involving this dietary constituent (1). Curcumin [1,7-bis(4-hydroxy-3-methoxyphenyl)-1,6-hepta-dien-3,5-dione] is a potent antioxidant derived from the spice turmeric. It exerts cancer chemopreventive efficacy in a wide variety of rodent models of carcinogenesis (2). In common with several other diet-derived polyphenols, curcumin possesses low systemic bioavailability (3). This pharmacoki-netic feature of curcumin, which has been observed across several species, is the corollary of poor absorption and avid metabolic conjugation and reduction (3, 4). Poor systemic availability mitigates against using curcumin in the preven-tion of malignancies distant from the gastrointestinal tract. In contrast, the low systemic bioavailability of curcumin would not curtail its development in the prevention of gastrointes-tinal malignancies, as curcumin distribution in the target tissue is, to a great extent, independent of systemic availability. Consistent with this notion oral curcumin has been shown to prevent malignancy in azoxymethane-induced colonic cancer model in rats (5) and to reduce adenoma burden in the ApcMin+ murine model of inherited colorectal cancer (6, 7). ApcMin+ mice are characterized by a mutation in the Apc gene mimicking the molecular defect underlying familial adenomatous polyposis in humans. The ApcMin+ model was used in the preclinical development of the cyclooxygenase-2 (COX-2) inhibitor celecoxib (8) and accu-rately predicted polyp-retarding activity in familiar adeno-matous polyposis patients (9). The mechanisms by which curcumin is thought to exert its chemopreventive efficacy include antioxidation, as reflected by a decrease in the level of the oxidative DNA adduct 3-(2-deoxy-h-di-erythro-pentafur-anosyl)-pyr[1,2-]-purin-10(3H)one (M1G; ref. 10) and by down-regulation of the enzyme COX-2 (11, 12). Expression of COX-2 mRNA and protein is increased in human colorectal adenomas and adenocarcinomas (13-15) compared with normal tissue, intimating the possibility of COX-2 inhibition as a strategy to intercept the development of colorectal cancer. Among other pharmacologic changes elicited by curcumin which have been considered to contribute to its chemopreventive efficacy are induction of apoptosis (16, 17) and antiangiogenesis (18). The concentrations of curcumin required to elicit biochemical changes germane to chemoprevention in experiments in vitro are in the 5 to 50 Amol/L range. Hence, for the development of curcumin as a potential colorectal cancer chemopreventive agent, it is of paramount importance to establish whether intestinal levels of curcumin in this concentration range are achievable in humans who receive oral curcumin, thus potentially eliciting pharmacologic changes which, when maintained over prolonged periods of time, might elicit chemoprevention. To test this hypothesis, patients with confirmed colorectal cancer received oral curcumin at 450, 1,800, or 3,600 mg per diem for 1 week before surgery, and levels of agent-derived species were determined in the peripheral circulation and in colorectal tissue obtained at resection surgery. We also explored whether metabolites of curcumin occur in the human colorectum. Furthermore, the hypothesis was tested such that oral consumption of curcumin precipitates changes in COX-2 levels and in redox status, as reflected by M1G adduct levels, in the colorectal mucosa. Levels of COX-2 protein and M1G adduct in tissue obtained at resection following 1 week of curcumin administration were compared with those in biopsy samples taken at diagnosis before administration of curcumin.
Materials and Methods
Patients and Tissue Collection. Twelve patients (5 female, 7 male, ages 47-72) with confirmed colorectal carcinoma of stages Dukes A (two patients), B (three patients), or C (seven patients) were recruited into the trial following approval by the local ethics committee. All patients gave written informed consent for the use of their tissues for the designated research project. Hematologic profiles, urinary levels of urea and electrolytes, and hepatic function were within the reference range defined by the laboratories of the University Hospitals of Leicester. None of the patients had preoperative radiotherapy or chemotherapy. Their drug history included antihyperten-sives (four patients), diuretics (five patients), and analgesics (five patients). None of the patients were on nonsteroidal anti-inflammatory drugs at the time of curcumin administration. Tumor location was the ascending/transverse colon (three patients), sigmoid colon (six patients), and rectum (three patients).
Colorectal tissue biopsy specimens taken at diagnosis weighed 6 to 40 mg (tumor biopsies) and 8 to 30 mg (normal tissue biopsies). The weight of the surgical tissue samples for pharmacodynamic analysis was 45 to 85 mg, that of samples for chemical analysis was 1.1 to 1.5 g. Tissues were placed in liquid nitrogen immediately after collection and kept at 80jC until analysis protected from light, and storage did not exceed 1 week. Previous work (4) established that curcumin is stable under these conditions in tissues.
Curcumin Formulation and Dose. Patients (four per dose level) received a standardized turmeric extract formulated in capsules (”Curcumin C3 complex,” Sabinsa Co., Piscataway, NJ). The capsule content of curcumin was confirmed by high-performance liquid chromatography (HPLC). Each capsule contained 450 mg of curcumin, 30 mg of desmethoxycurcumin, and 20 mg of bisdesmethoxycurcumin. Dose levels were 1, 4, or 8 capsules per day, translating into 450, 1,800, or 3,600 mg of curcumin daily, for 7 days before surgery. Samples of peripheral blood were taken 1 hour post dose, and colectomy was done 6 to 7 hours after the last dose of curcumin.
Analysis of Curcumin and Curcumin Conjugates. Samples of tissues and plasma were extracted and analyzed by HPLC for curcumin and its major metabolites curcumin sulfate, curcumin glucuronide, hexahydrocurcumin, and hexahydro-curcuminol, as described by previously (3, 4). Recovery of curcumin was 81 F 2% from plasma and 76 F 3% and 75 F 6% from colorectal tumor tissue and normal colorectal mucosa, respectively. Authentic curcumin glucuronide and curcumin sulfate were generated by incubation of curcumin with rat liver microsomes and cytosol, respectively, with appropriate cofactors (4). Authentic hexahydrocurcumin and hexahydrocurcuminol were generated by reduction of curcumin with sodium borohydride (3). Identification was done by HPLC cochromatography with standard materials and by mass spectrometry using a Quattro Ultima Platinum Mass Spectrometer (Micromass, Manchester, United King-dom). For mass spectral analysis, samples (10 AL) of eluate obtained from the HPLC column containing suspected curcumin-derived species were dried and solubilized in acetonitrile/water (7:3) and injected into the mass spectrom-eter using a back flow of 70:30 acetonitrile/water at 50 AL/min (Waters Alliance 2695 HPLC pump) using desolvation and source temperatures of 200jC and 120jC, respectively. The mass spectrometer was tuned up to each authentic agent before sample analysis. Analysis involved a scan of 40 to 600 m/z. Tandem mass spectrometry was used to fragment molecular ions into product ions; argon was the collision gas.
Analyses of COX-2 Protein and M1G Adducts. COX-2 protein in colorectal tissue was determined by Western blotting using an anti-COX-2 polyclonal antibody (Santa Cruz, TX) with enhanced chemiluminescence detection as described previously (19). Protein loading was 400 Ag per lane. DNA was extracted from tissue and M1G adduct levels were measured by immunoslot blot, using monoclonal anti-M1G antibody provided by Prof. Lawrence Marnett (Vanderbilt University, TN) as described previously (20).
Results
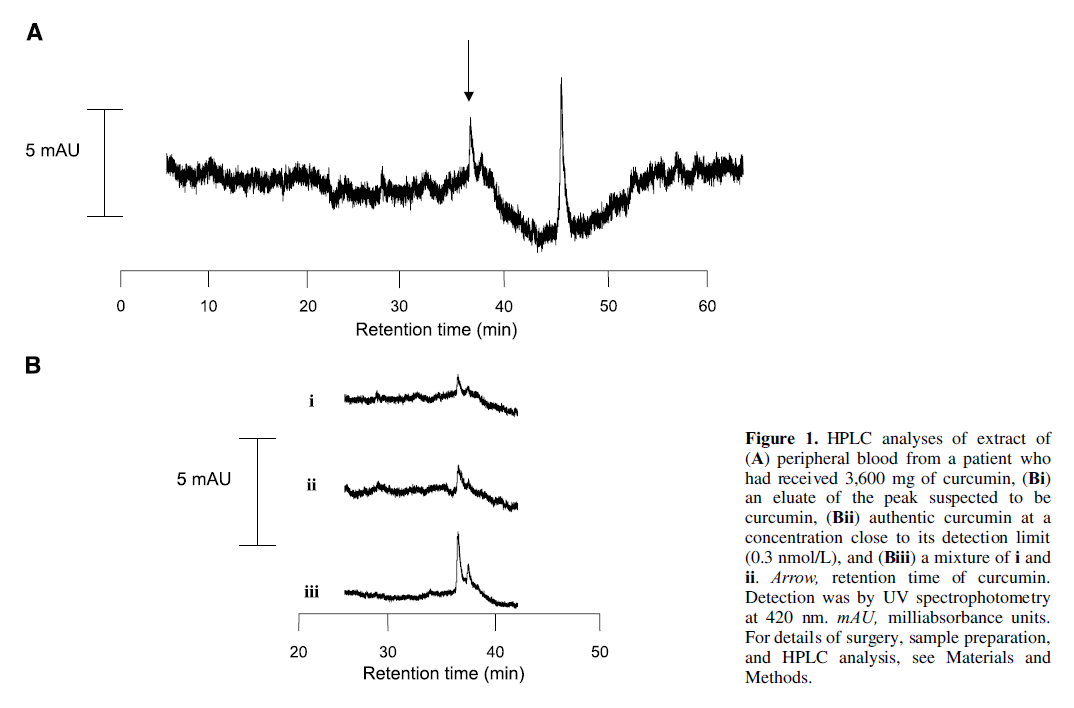
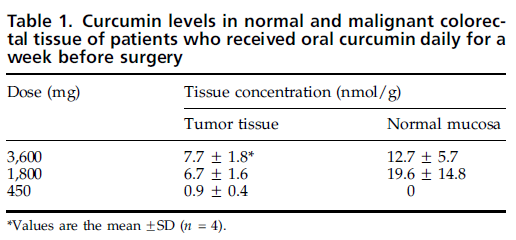
Identification of Curcumin and its Metabolites in Blood and Colorectal Tissue. Samples of extracts of plasma obtained from the peripheral circulation or of normal or malignant colorectal tissue were subjected to HPLC analysis. Plasma from one of the patients on the highest dose of curcumin (3,600 mg) afforded a peak coeluting with authentic curcumin (Fig. 1). This peak was not found in plasma from the other patients at this or the two lower dose levels. An abundant peak with the retention time of 38 minutes, coeluting with curcumin, was found in extracts of normal and malignant colorectal tissue in patients at all three dose levels (see, e.g., in Fig. 2). Confirmation of identity of this species as curcumin was achieved by cochromatography with authentic material of an extract of the eluate containing the peak constituent, and by mass spectrometric analysis. Mass spectra of the eluate of tissue extracts containing this peak were characterized by a predominant molecular ion at m/z 367 and a diagnostic on source collision induced a dissociation fragment at m/z of 325, consistent with the spectrum of authentic curcumin. Curcumin levels in the plasma were above the limit of detection (f0.3 nmol/L), but below the limit of quantitation (3 nmol/ L). Levels of curcumin in normal and malignant colorectal tissue ranged from 7 to 20 nmol/g tissue (Table 1). Normal mucosa from the caecum and ascending colon contained more curcumin than normal mucosa from the transverse, splenic flexure, and descending colon. In patients who had received 1,800 or 3,600 mg of curcumin, the concentration of curcumin measured was 21.7 F 8.2 and 6.8 F 3.7 nmol/g in the right and left colon, respectively (mean F SD, n = 4 patients per dose level). This difference was not reflected by curcumin levels in tumor tissue originating from differential sites of the bowel. Curcumin metabolites were not detected in the plasma. Extracts of colorectal mucosa of seven of the eight patients who received 1,800 or 3,600 mg curcumin yielded an HPLC peak which coeluted with curcumin sulfate, and tissue extracts from two patients on the highest dose exhibited a peak coeluting with curcumin glucuronide (Fig. 2). Unambiguous identification of these species was achieved by mass spec-trometry which afforded the molecular ions of m/z = 543 and 447 which when subjected to tandem mass spectrometry gave product ion spectra consistent with mass spectra for authentic curcumin glucuronide and curcumin sulfate. Curcumin…
…conjugates possess absorbance coefficients similar to those of curcumin (3), and semiquantitative interpretation of the HPLC traces suggested that the conjugates were present at concen-trations near 1 pmol/g tissue. Presence of curcumin conjugates in the intestinal mucosa is consistent with the finding that curcumin undergoes avid glucuronidation and sulfation in suspensions of microsomes and cytosol, respectively, from the intestine of humans and rodents (4). Curcumin also undergoes metabolic reduction to hexahydrocurcumin and hexahydro-curcuminol (3). These metabolites were undetectable in extracts of intestinal tissue.
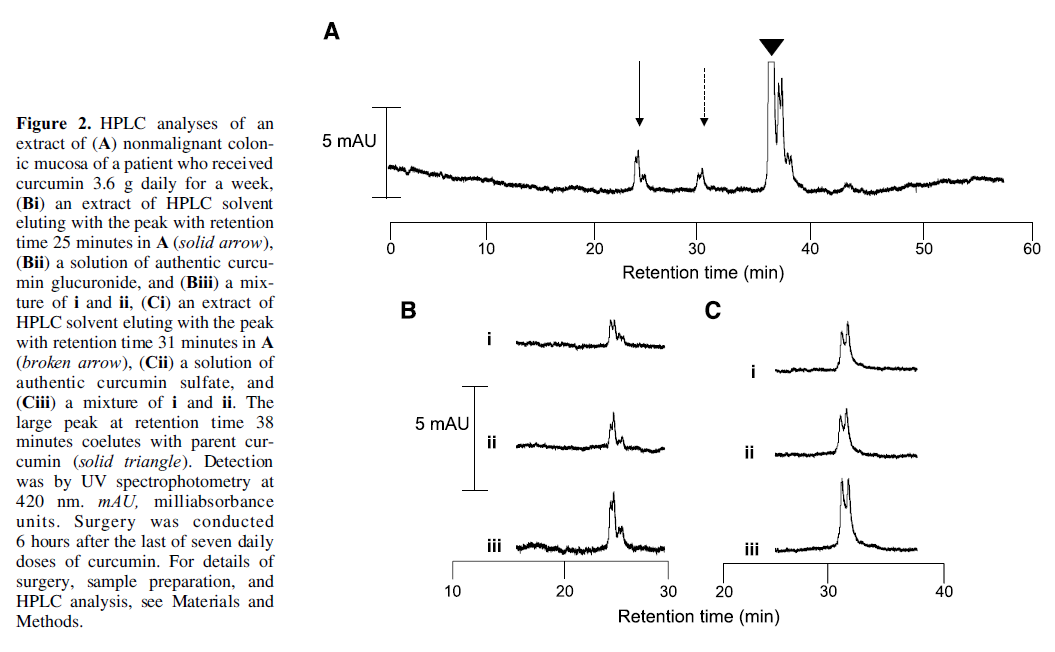
Effect of Curcumin on Colorectal COX-2 and M1G Levels. The potential pharmacodynamic activity of orally ingested curcumin in the colorectum of cancer patients was tested by assessment of its effect on the expression of COX-2 protein and on levels of M1G. COX-2 and M1G levels in surgical colorectal tissue samples were compared with levels in biopsy specimens obtained at the time of diagnosis. COX-2 was undetectable in normal colorectal tissue, but present in malignant colorectal tissue (Fig. 3), consistent with previous studies (21 – 23). Curcumin did not seem to reduce COX-2 expression in malignant colorectal tissue.
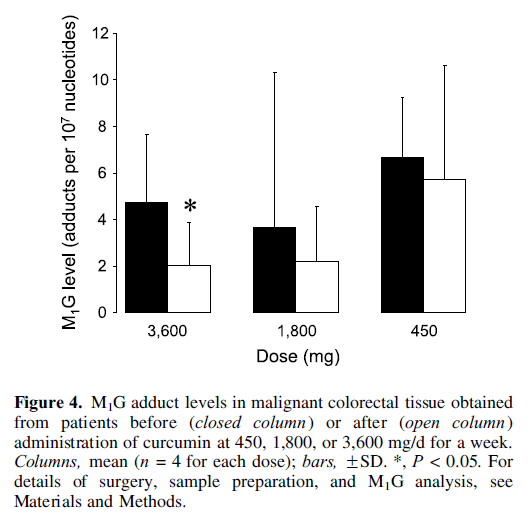
M1G adduct levels in normal and malignant colorectal tissue were 2.3 F 1.1 and 4.8 F 4.9 per 107 nucleotides (n = 15, P < 0.05 by ANOVA), respectively, thus 2.5-fold higher in malignant tissue compared with normal tissue. Whereas administration of curcumin did not affect M1G levels in normal colorectal mucosa, it caused a decrease in adduct levels in malignant colorectal tissue (Fig. 4). In the case of the highest cucumin dose, the difference between samples obtained pretreatment and post-treatment reached borderline significance (P < 0.05). To explore the relevance of the observed difference further, we investigated whether M1G levels were affected by the specific manner in which tissue samples were obtained. Pretreatment biopsy samples consisted predominately of malignant tissue obtained from the surface of the tumor. In contrast, samples obtained at surgery consisted of a ''wedge'' of tissue including tumor core. It was deemed conceivable that samples taken from the edge or the middle of the tumor could differ in M1G levels because of differences in exposure of tissue to oxidants in the fecal stream or of variation in blood supply. To test this hypothesis, M1G adduct levels were measured in three patients who had not received curcumin. M1G levels in preoperative biopsy specimens were 4-fold higher than those obtained from surgically obtained tumor core, and M1G levels in postopera-tive tumor edge were approximately twice as high as in tumor core obtained postsurgery (data not shown). Thus, it would seem that differences in origin of tumor sample between preoperative (and hence pretreatment) and postoperative (post-treatment) specimens could, at least in part, explain differences in M1G levels, which might in turn obfuscate any effect of curcumin. It is important to note that the effect of curcumin on colorectal M1G levels was borderline significant (P < 0.05) only in patients who had received the highest dose. If the variability in M1G levels between pretreatment and...
…post-treatment samples were predominantly due to the spatial diversity in sample source, one would expect the pretreatment and post-treatment difference in M1G levels to be of a similar order of magnitude in all three dose groups. Yet a marked discrepancy in pretreatment and post-treatment M1G levels was not seen for the 450 and 1,800 mg dose groups. Thus, it seems reasonable to draw the tentative conclusions that curcumin consumption did indeed cause a decrease in M1G levels in colorectal malignant tissue and that differences in M1G levels related to sampling technique were unlikely to confound the effect of curcumin. With a larger sample size, the dose of 1.8 g might actually have achieved a statistically significant reduction of M1G levels. Thus, although this study did not establish the minimal dose which decreased M1G levels (i.e., ”minimal effective dose”), we tentatively surmise that the minimal effective dose level might be >0.45 g and perhaps near 1.8 g.
Discussion
The results outlined above suggest that levels of curcumin achieved in humans after regular oral intake of 3,600 mg of curcumin furnish drug levels in the gastrointestinal tract which elicit pharmacodynamic changes. This novel conclusion supports the body of evidence, which advocates the further clinical development of curcumin as a colorectal cancer chemopreventive agent. The lack of quantifiable curcumin in the plasma observed here, even after a dose as high as 3,600 mg is consistent with recent clinical reports, in which oral doses of 30 to 180 mg curcumin failed to establish detectable plasma levels (24), and doses of 4,000 to 12,000 mg yielded curcumin peak levels of only f0.5 to 2 Amol/L within 1 hour of administration (25). Furthermore, in a recent clinical phase I study doses up to 3,600 mg curcumin were well tolerated and furnished only trace amounts of parent compound in the blood, but measurable concentrations of curcumin in the feces and of parent compound plus conjugate metabolites in the urine (26). Another conclusion of the work presented here is that products of metabolic curcumin conjugation are present in the colorectum of humans who have ingested curcumin, but that quantitatively these metabolites contribute only to a very minor extent to the overall colorectal load of curcumin-derived species. This finding is consistent with the notion that pharmacologic effects of curcumin exerted in the colorectum are likely to be caused by the parent compound and not by its metabolites.
In a recent study in ApcMin+ mice, levels of curcumin in the intestinal mucosa were compared with its ability to decrease adenoma formation (7), down-regulate intestinal COX-2 expression and decrease the level of the M1G adduct in murine intestinal tissue2. The results intimate that curcumin doses which result in intestinal mucosal levels in the 100nmol/g range, are required to reduce the adenoma burden in mice, and that chemopreventive efficacy is reflected by significant decreases in murine adenomatous COX-2 expres-sion and M1G levels. The data described in the results presented above allow extrapolation of these insights to humans. The curcumin levels observed in the human color-ectum after consumption of daily doses of 1,800 or 3,600 mg as described here are of an order of magnitude which has been shown to elicit pharmacologic activity in cells in vitro (12, 16-18), although they are only about a tenth of the levels which have been associated with retardation of adenoma format on in the ApcMin+ mouse model (7). Nevertheless, the antioxida-tive changes in malignant colorectal tissue, as adjudged by M1G levels in humans who ingested 3,600 mg curcumin, seem to be quantitatively similar to the extent of reduction of M1G levels which accompanied the chemopreventive efficacy of curcumin at 0.2% in the diet (equivalent to 300 mg/kg per day) in ApcMin+ mice. The apparent antioxidative equivalence for curcumin in the intestinal tract between ApcMin+ mice and humans as reflected by M1G levels is not surprising in the light of the fact that the curcumin dose in humans equivalent to the 0.2 % dietary concentration used in mice, when calculated on the basis of equivalent body surface area (900 mg/m2), would be 1.6 g per person daily, assuming a body surface area of 1.8 m2 accompanying a body weight of 70 kg (26), a dose similar to that shown to be efficacious here. Whilst ingestion of curcumin for a week affected M1G levels in patients’ colorectal tissue, it was insufficient to decrease COX-2 protein expression in this tissue. This result contrasts with the observation in ApcMin+ mice, in which curcumin consumption, albeit for the postweaning lifetime, drastically reduced COX-2 levels. This reduction may have been the corollary of curcumin-induced retardation of adenoma development. It remains to be established whether ingestion for a term longer than a week would reduce COX-2 protein expression in humans.
Taken together, the results presented here and elsewhere suggest that whilst orally ingested curcumin has low systemic availability, it furnishes sufficient levels in the human intestinal tract to cause pharmacodynamic changes commensurate with intestinal chemoprevention. The low systemic availability of curcumin might be considered a disadvantage because it precludes the use of curcumin as a chemopreventive agent for target organs distant from the gastrointestinal tract. In accordance with this notion, a very recent study suggests that consumption of curcumin by patients at the doses described here results in levels of the agent in normal and malignant liver tissue, which are insufficient to exert pharmacologic activity (27). In contrast, the concentrations of curcumin achieved in the colorectal mucosa as outlined above are consistent with levels needed to exert chemopreventive activity. The ”negative targeting” of curcumin (i.e., its lack of ability to reach sites removed from the loci of its absorption and excretion) could be a considerable advantage, minimizing potentially detrimental exposure of other organs. All of this evidence suggests that the further evaluation of curcumin as a colorectal cancer chemopreventive agent may be propitious. The results described here in concert with a previous study (27) suggest that a daily dose of 3,600 g is safe in humans. This dose has been shown here to furnish agent levels in the target organ,…
…which may be adequate to elicit antioxidative changes
commensurate with long-term benefit. All of this data is
buttressed by extensive mechanistic information on curcumin
(28). Thus, the preliminary findings presented here provide
some rationale to consider progression of curcumin into
phase II evaluation as a cancer chemopreventive agent in
patients at risk of colorectal cancer, such as those with
familial adenomatous polyposis.
References
- Omenn GS. Chemoprevention of lung cancer: the rise and demise of h-carotene. Annu Rev Public Health 1998;19:73 – 99.
- Kelloff JS, Crowell JA, Hawk ET, et chemopreventive drug development: clinical development plans II. J Cell Biochem 1994;26S:54 – 71.
- Ireson CR, Orr S, Jones DL, et al. Characterization of metabolites of the chemopreventive agent curcumin in human and rat hepatocytes and in rat plasma and evaluation expression. Cancer Res 2001;61:1058 – 64.
- Ireson CR, Jones DJL, Orr S, et al. Metabolism of the cancer chemopreventive agent curcumin in human and rat intestine. Cancer Epidemiol Biomarkers Prev 2002;11:97 – 104.
- Rao CV, Rivenson A, Simi B, et al. Chemoprevention of colon carcinogenesis by dietary curcumin, a naturally occurring plant phenolic Cancer Res 1995;55:259 – 66.
- Mahmoud NN, Carothers AM, Grunberger D, et al. Plant phenolics decrease intestinal tumours in an animal model of familial adenomatous polyposis. Carcinogenesis 2000;21:921 – 7.
- Perkins S, Verschoyle RD, Hill KA, et al. Chemopreventive efficacy and pharmacokinetics of curcumin in the Min/+ mouse, a model of familial adenomatous polyposis. Cancer Epidemiol Biomarkers Prev 2002;11:535 – 40.
- Jacoby RF, Seibert K, Cole CE, et al. The cyclooxygenase-2 inhibitor celecoxib is a potent preventive and therapeutic agent in the min mouse mode of adenomatous polyposis. Cancer Res 2000;60:5040 – 4.
- Steinbach G, Lynch PM, Phillips RKS, et al. The effect of celecoxib, a cyclooxygenase-2 inhibitor, in familiar adenomatous polyposis. N Engl J Med 2000;342:1946 – 52.
- Sharma RA, Ireson CR, Verschoyle RD, et al. Effects of dietary curcumin on glutathione S -transferase and malondialdehyde DNA adducts in rat liver and colon mucosa: relationship with drug levels. Clin Cancer Res 2000;7: 1452 – 8.
- Huang MT, Lysz T, Ferraro T, et al. Inhibitory effect of curcumin on in vitro lipoxygenase and cyclooxygenase activities in mouse epidermis. Cancer Res 1991;51:813 – 9.
- Plummer SM, Holloway KA, Manson MM, et al. Inhibition of cycloox-ygnease-2 expression in colon cells by the chemopreventive agent curcumin involves inhibition of NF-B activation via the NIK/IKK signalling complex. Oncogene 1999;18:6013 – 20.
- Tsujii M, Kawano S, DuBois RN. Cyclooxygnase-2 expression in human colon cancer cells increases metastatic potential. Proc Natl Acad Sci U S A 1994;94:336 – 40.
- Kargman SL, O’Neill GP, Vickers PJ, et al. Expression of prostaglandin G/H synthetase-1 and -2 protein in human colon cancer. Cancer Res 1995;55:2556 – 9.
- Oshima N, Dinchunk JE, Karman SI, et al. Suppression of intestinal polyposis in APC y716 knockout mice by inhibition of cyclooxygnase-2 (COX-2). Cell 1996;87:803 – 9.
- Kuo ML, Huang TS, Lin JK. Curcumin, an antioxidant and anti-tumour promoter induces apoptosis in human leukaemia cells. Biochim Biophys Acta 1996;1317:965 – 1000.
- Kawamori T, Lubet R, Steele VE, et al. Chemopreventive effect of curcumin, a naturally occurring anti-inflammatory agent, during the promotion/ progression stages of cancer. Cancer Res 1999;59:597 – 601.
- Arbiser JL, Klauber N, Rohan R, et al. Curcumin is an in vivo inhibitor of angiogenesis. Mol Med 1998;4:376 – 83.
- Yoshimatsu K, Golijanin D, Paty PB, et al. Inducible microsomal prostaglandin E synthase is overexpressed in colorectal adenomas and cancer. Clin Cancer Res 2001;7:3971 – 6.
- Leuratti C, Singh R, Lagneau C, et al. Determination of malondialdehyde-induced DNA damage in human tissues using an immunoslot blot assay. Carcinogenesis 1998;19:919 – 24.
- Dimberg JA, Samuelsson A, Hugander A, et al. Differential expression of cyclooxygenase 2 in human colorectal cancer. Gut 1999;45:730 – 2.
- Sheehan KM, Sheahan K, O’Donoghue DP, et al. The relationship between cyclooxygenase-2 expression and colorectal cancer. JAMA 1999; 282:1254 – 7.
- Wiese FW, Thompson PA, Warneke J, et al. Variation in cyclooxygenase expression levels within the colorectum. Mol Carcinog 2003;37:25 – 31.
- Sharma RA, McLelland HR, Ireson CR, et al. Pharmacodynamic and pharmacokinetic study of oral Curcuma extract in patients with colorectal cancer. Clin Cancer Res 2001;7:1894 – 900.
- Cheng AL, Hsu CH, Lin JK, et al. Phase I clinical trial of curcumin, a chemopreventive agent, in patients with high-risk or premalignant lesions. Anticancer Res 2001;21:2895 – 900.
- Freireich EJ, Gehan EA, Rall DP, et al. Quantitative comparison of toxicity of anticancer agents in mouse, rat, hamster, dog, monkey and man. Cancer Chemother Rep 1966;50:219 – 44.
- Garcea G, Jones DJL, Dennison AR, et al. Detection of curcumin and its metabolites in hepatic tissue and portal blood of patients following oral administration. Br J Cancer 2004;90:1011 – 5.
- Gescher A, Sharma RA, Steward WP. Cancer chemoprevention by dietary constituents: a salutary tale of failure and promise. Lancet Oncol 2001;2:371 – 9.






